
How long have you been using e.max and what is your experience with it?
I have used e.max extensively over the past 12years – as long as I have worked in South Africa – and was one of the first people to use it. I’ve done almost six thousand restorations using e.max and haven’t found any other material that matches up to it. Its longevity and aesthetics is impressive.
What are your key reasons for choosing to use e.max
In the past dentists have had to compromise on materials that look good but don’t last very long. e.max restorations have both beauty and long life. It also allows us to apply minimally invasive protocols as a more conservative approach to restorations. I can restore the teeth without having to destroy them first. It fits our need in every way and is an absolute win-win option. IVOCLAR has managed to create a material that adapts to each patient – colour, aesthetics… etc. It fits seamlessly into where dentistry is going – from analogue to digital – the adaptation has been done – and Ivoclar is ahead of the game.
Longevity and aesthetics are the key cornerstones in dentistry – we always had to compromise…. Now we have the best of both worlds with e.max.
In the 12 years I have been working with e.max I have had the time to see and evaluate the cases…..and I am even more enthusiastic now I can see the longevity!!
I love its versatility – I can do the front and back of mouth and implants.
Ivoclar has had the opportunity to develop something in a way that fits our needs in a big way – it is an outstanding option.
The materials are designed to fit every case – no longer is it necessary to compromise on lifespan in favour of quality.
Because no two cases are the same, Ivoclar has managed to create a material that adapts to each patient – colour, aesthetics… etc.
Some dentists do resist changes but I have adapted, from single teeth to full mouth rehabilitations. I run an aesthetic and restorative practice. It fits into where dentistry is going – from analogue to digital – the adaptation has been done – and Ivoclar is ahead of the game…
The versatility of materials is exciting, I can use an ingot hand-made (wax and press) or milled in a block, design CAD and CAM and mill!
Very few materials have long term research to back up long-term claims – I have confidence due to the success I have achieved over the years, supported by the clinical research.
I love the predictability of the material – successful delivery, treatment and longevity benefits both me and the patient financially and brings credibility and satisfaction.
Dr Bowes is a Fellow of the International Congress of Oral Implantologists; practised in London for 23years and in 2010 founded the South African Academy of Aesthetic Dentistry. He runs a private practice in Cape Town, focussed on Aesthetic and Complex Restorative Dentistry. He is a member and registered speaker for the ITI – International Team for Implantology. As Founder and past president of the South African Academy of Aesthetic Dentistry, he has pioneered the development of Digital Smile Design in South Africa, enabling dentists to develop a smile which fits both aesthetic and functional needs for each individual. As a DSD World Master and Instructor, he lectures and teaches both in Southern Africa and internationally. He is passionate about minimally invasive treatment and has introduced IAS – Intelligent Aligner Systems to South Africa, running courses to teach fellow dentists. Mark has recently been invited to be a silver member of the prestigious group Styleitaliano and an honorary global ambassador for @slowdentistry. He is an ambassador of the Humble Smile Foundation – a global group of dental and development professionals who passionately promote oral health and prevent oral disease as an integral part of children’s well-being.
Click here for more e.max product info and IVOdeals.

I have been using e.max in my practice for almost 15years and I can say in all confidence that it surpasses any other material I have ever used before. It’s more superior as it’s the most stable and versatile material for the job at hand. I can go home and sleep well at night knowing I do not have to worry about the work done, confident that no problems will be experienced.
I use it mainly for crown and bridge work, full rehabilitation cases and have more recently moved into doing a large amount of inlays and onlays, implant based crowns … pretty much everything actually - there really is nothing we can’t use it for!
More and more we get patients who come in and demand “the real e.max material”. So much so that we use e.max stickers to put on their invoices and cards to prove to them we have used it. I find patients nowadays are well prepared and educated and come to us having done their homework and well aware of all the options available to them. They do not want Zirconia at all. We last saw this with daVinci Porcelain; patients knew about it and asked for it. Now they ask for e.max.
The strength angle is overrated; there are stronger materials out there, but for me, why I find it superior for the job is that it’s an all-rounder – combining strength, versatility, aesthetics and bondability. When you learn how to properly process and bond it, what more do you want!? And of course it’s proven, not just in my hands, but in many, many published reports.
I conduct a lot of CADCAM training courses, and in fact am doing an anterior course this week, and I always tell doctors on my courses how essential it is to have e.max as a staple in their practice and we teach and show them how to manage and process it and tell them that they can advocate it with 100% confidence. I tell them “e.max is the GO TO block!”
Dr Vikash Naidoo graduated from the University of Witwatersrand in 2001, and entered private practice soon after qualifying. Very early on in his career he showed a flair for cosmetic dentistry, and soon thereafter incorporated the art of computerized cosmetic dentistry into his practice. His passion for the computerized cosmetic world of dentistry is such that he has become an international certified CEREC trainer, and derives great satisfaction in training dentists who are new to the CEREC community.
Being invested in computerized dentistry has allowed Vikash to travel the globe, ensuring that he is at the cutting edge of the latest developments in this digital area. Technology has rapidly progressed over the past decade, making dentistry easier, precise, highly efficient and less traumatic, a doctrine Vikash embraces completely. Vikash realised that cosmetically enhancing a patient’s smile, is in most cases only one part of the equation, resulting in him becoming an accredited Dermal filler practitioner, allowing a holistic approach to facial aesthetics. He also has completed a number of post graduate surgical implant courses through the much respected Implant Academy, placing him in a perfect position to be able to complete an excellent standard of comprehensive care. Dr Vikash Naidoo is an Executive member of the South African Academy of Cosmetic Dentistry (SAACD), and participating member of the International Society of Clinical Dentistry (ISCD), South African Dental Association (SADA) and Health Professions Council of South Africa (HPCSA).
Click here for more e.max product info and IVOdeals.

How long have you been using e.max?
I have worked with bonding ceramics for 34yrs; prior to e.max I used EMpress 1 and EMpress 2.
e.max revolutionised the dental industry, mainly due to its strength and versatility. I have been using it since its arrival on the South African scene, and it has added exceptional value both to my practice and to dentistry as a whole!
It seems to require 30yrs for a paradigm shift to occur in dentistry and this has now happened, with bonded ceramics being adopted as the treatment of choice in indirect restorations. It’s very exciting - especially with e.max!
What do you like most about using the product?
I like the fact that you can use e-max equally well for veneers, inlays, onlays as well as full crowns. So it’s one product for very many different applications. Being able to use the same ceramic throughout allows for conformity of colour and texture which maximises aesthetic outcomes. With e.max offering copings in five different translucency levels each with multiple shades, this allows even more versatility – catering for all needs, no matter the colour of the underlying tooth structure. It’s just like a box of chocolates – sometimes I feel like a chef…. you can pick and choose and create the proper recipe for a particular situation for ultimate perfection!
Also it gives you the option of going monolithic for strength, or a layered technique can be utilized for better aesthetics – incredible flexibility in aesthetics…. Just brilliant! Bonded ceramics is definitely my preferred choice as opposed to conventional cemented crowns.
What I really like about e.max and bonded ceramics is that it is very strong even in thin layers, ideal for veneers and table top overlays. It’s minimally invasive, as opposed to the traditional methods. With patients getting older and living longer we need to do more minimally invasive treatments and also treatments that help teeth last much longer than before - they need to last a lifetime! The e.max durability is the perfect solution.
Furthermore, depending on the application and design it can be luted with fully adhesive techniques, self-adhesive techniques or conventional cementation techniques. Due to these flexible cementation options we are able to offer reliability and ease of use for the appropriate situation.
And the fact that it is available in the analogue press technique or for the digital CAD Cam applications, is great.
Another positive with ceramic restoration is that it’s EASY to use; it can be prepped with traditional hydrofluoric acid plus silane or the new impressive and convenient, “monobond etch and prime” solution.
It’s EASY to adjust and polish, even intra-orally after cementation, should it be required.
What would you like to share with other dentists about using e.max?
Ultimately what sells it for me after all my years of using e.max in my practice, is the feeling I get when patients who had major restorations done previously, come in for check-ups years down the line and I look in their mouths only to see a perfect dentition with nothing needing to be done. e.max is so durable that it’s almost unnecessary to have wasted their time for a follow up examination, as I can almost predict even before examining them, that everything will be in great shape. Nevertheless it always gives me a kick to be able to give them a clear bill of health…. to say nothing needs to be done today”….Your teeth are perfect! Any problems are usually very minor in the form of a small chip or something similar, which can easily be repaired and polished intraorally to continue the durability and longevity!
Essentially e.max equates to COST EFFECTIVE dentistry…. The return on investment is huge and long term – very few, problems if any occur down the line – actually it is not only FINANCIALLY cost effective but most importantly is BIOLOGICALLY cost effective – as by using minimally invasive treatment options and keeping the mouth in tip top condition, it maintains overall body health!
Dr Effting graduated at the University of Witwatersrand as the Best All Round Student and is senior dentist and clinical director of Hout Bay Dental Studio in the Western Cape. With nearly 40yrs experience, he has a particular interest in mercury-free, minimally invasive dentistry with wide experience in implantology and in treating patients in a holistic manner. He is a founding member and President of the South African Academy of Aesthetic Dentistry and Fellow of the International Team of Implantology. In his spare time he is a keen sportsman with a particular love of cycling.
Click here for more e.max product info and IVOdeals.

Modern implant rehabilitation has become a computer-driven process, where CBCT imaging, surgical planning and prosthetic design software all allow the implementation of a digital workflow (Lerner et al. 2021). This workflow does not only help the practitioner execute the planned implant easily , but also increases the predictability and clinical success of osseointegration. It also aid in immediate loading protocols along the biological developments of fusing implant surfaces to grafted bone and peri-implant supporting structures (Adell et al. 1981; Albrektsson et al. 1986).
Nevertheless, at the end of this digital process, all the intended prosthetic design elements cannot account for the occlusal loads that occur during function on a newly installed, rigid, immobile, and unforgiving implant-supported prosthesis. Complication rates in implant prosthodontics exceed those of traditional tooth-supported restorations (Sailer et al. 2018), which necessitates following an occlusal scheme to combat destructive occlusal forces that often damage implant restorations.
Generally, applied occlusal forces are controlled through pulpal and periodontal ligament (PDL) mechanoreception and proprioception, and are somewhat neutralized by the periodontal structures (Madani et al. 2017; Dario 1995). Unlike natural teeth, the absorption of masticatory forces through osseoperception is reduced with implant-supported prostheses, due to the absence of a periodontal ligament (Madani et al. 2017; Dario 1995). While teeth can move apically within the socket about 50 to 100 µm, apical implant movement is limited to only 3 to 5 µm (Roque 2017). Hence, the occlusal material on an implant-supported crown bears the entire applied occlusal force, and can affect the structural integrity of both the abutment and implant body, as well.
Typically, an implant-supported prosthesis is delivered with an implant-protective occlusal scheme (IPO), developed with shim stock and very thin articulating paper. The implant occlusal surface is theoretically sub-occluded from the opposing occlusal surface by 25 µm, to prevent occlusal force overload during a normal strength mandibular closure into maximum intercuspation (Bozhkova 2016; Chaithanya et al. 2019; Luo et al. 2020).
Despite the widespread belief that an IPO provides adequate control over occlusal forces, occlusion related mechanical complications in implant-supported prosthesis remain common (Elemek et al. 2020; Papaspyridakos et al. 2020; Lerner et al. 2020; Sailer et al. 2018; Shen et al. 2018; Pjetursson et al. 2018; Drago 2016; Wittneben et al. 2014; Fischer et al. 2013; Pjetursson et al. 2012; Bozini et al. 2011; Jemt 2006), as long term survival studies indicate that mechanical complication rates in implant -supported prosthesis supersede those of natural teeth. (Elemek et al. 2020; Papaspyridakos et al. 2020; Lerner et al. 2020; Sailer et al. 2018; Shen et al. 2018; Pjetursson et al. 2018; Drago 2016; Wittneben et al. 2014; Fischer et al. 2013; Pjetursson et al. 2012; Bozini et al. 2011; Jemt 2006). Therefore, compared to tooth-supported prosthesis, implant rehabilitations require meticulously adapted occlusion because the implant-supported prosthesis lacks resiliency, elasticity, and forgiveness (Lerner 2020).
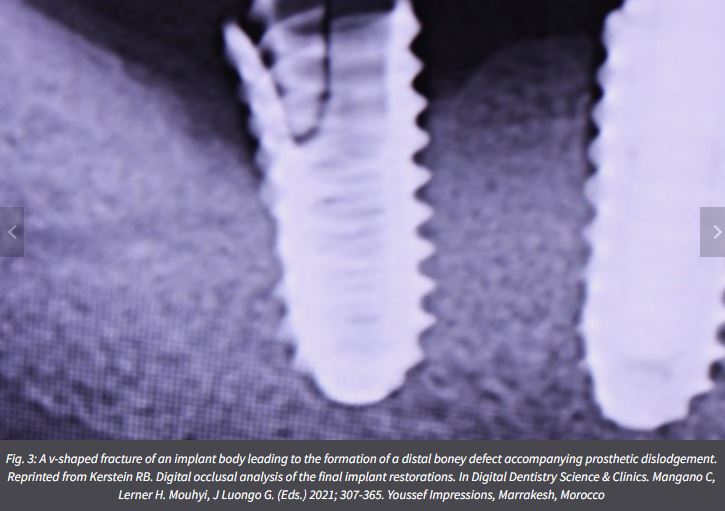
There are many known types of implant complications that result from increased occlusal overload (Adell et al. 1981; Albrektsson et al. 1986; Esposito et al. 1998; Balshi 1996), which can elevate peri-implant crevicular fluid levels, compromising peri-implant tissue health while leading to possible bone loss. The frequent mechanical complications include:


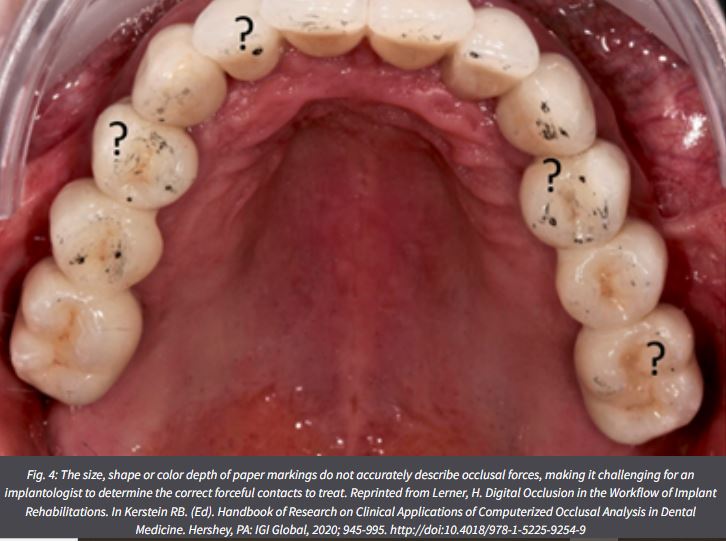
A major contributor to a common occlusion-related mechanical complications is the clinical use of analog traditional occlusal indicators, such as articulating paper/foil/strips/horeshoes, shim stock “hold”, occlusal wax imprints, silicone imprints, and articulated casts (both stone and virtual) (Qadeer & Sarinnaphakorn 2020) . Studies have shown that articulating paper specifically, is incapable of measuring occlusal forces (Balshi 1996; Qadeer et al. 2012; Saad et al. 2008; Carey et al. 2007; Bozhkova 2020), leaving the clinician to adjust occlusion by “subjectively interpreting” the articulating paper marks. Unfortunately, this contact selection method is highly prone to error and fails to reliably control force levels (Basson et al. 2020; Sutter 2017; Kerstein & Radke 2013). Studies have shown that by relying on the visual detection of articulating paper marks, dentists select incorrect contacts 87-95% of the time (Basson et al. 2020; Sutter 2017; Kerstein & Radke 2013).
Adding computerized occlusal analysis (T-Scan 10 Novus, Tekscan, Inc., Norwood, MA, USA) when adjusting occlusion in cases definitive implant restorations or in cases of immediate loading, helps ensure a predictable targeting of problematic occlusal loads when adjusting occlusion (Lerner 2020). These problematic occlusal loads include premature contacts and excessive contact forces that can de-stabilize an implant restoration. Several digital occlusal tools exist that can aid in occlusal adjustments like Accura (Dmetec Co, Ltd, Seoul, South Korea) , Occlusense (Gmbh Bausch, Germany), and T-Scan , the latter being the most clinically tested device (Sutter 2019).
Many studies have been conducted on T-Scan (Qadeer et al. 2020) that have verified its accuracy in detecting occlusal problems (Koos et al. 2010), its force reproducibility (Harty et al. 2006; Koos et al. 2010; da Silva Martins et al. 2014; Kerstein & Radke, 2022), its time quantification (Koos et al. 2012), and its clinical effectiveness in many areas of patient occlusal care (Qadeer et. al. 2020). Many digital occlusion T-Scan protocols exist in Prosthodontics, Dental Implants, the Digital Workflow, TMD, Posturology, Orthodontics, Periodontics, Occlusal Diagnosis, Aesthetic Dentistry, Tooth Hypersensitivity, Mandibular Orthosis, Occlusal Adjustments, and Patient Education (Kerstein 2020).
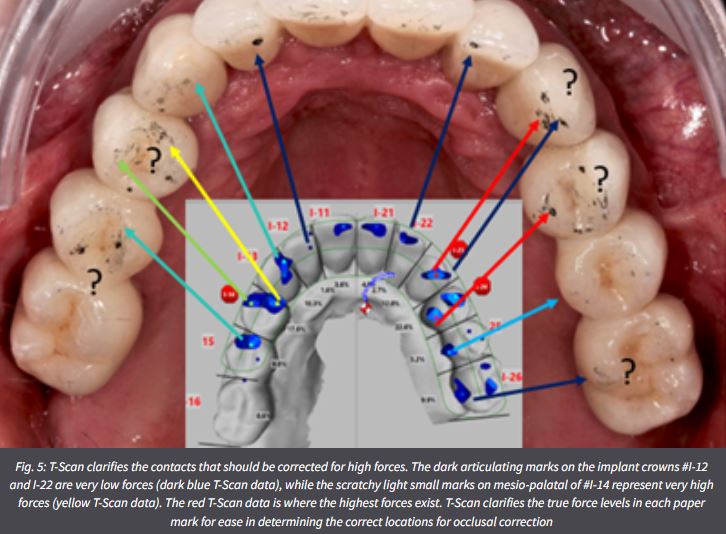
Digital occlusal indicators like T-Scan dynamically records and displays the occlusion time (OT), disclusion time (DT), the relative force % distribution, the intensity of 256 relative occlusal forces and their duration, and the timing order of all occlusal contacts, as they each occur inter-occlusally during functional mandibular movements (Kerstein 2020).Such indicators bring objective data to the process of occlusally adjusting an implant restoration, whether the case is full-arch implant supported prosthesis, a removable overdenture, a segmental implant restoration, or a single unit (Aradya et al. 2022; Mangano et al. 2021; Kuder et al. 2017; Ma et al. 2016; Cotruţă et al. 2015). Regardless of the clinician’s desired occlusal scheme (Implant Protected; Anterior Guided, or Balanced), the digital indicator can guide the contacts selected for corrective adjustment where the case installation outcomes are quantifiably improved compared to those obtained with subjectively interpreted, non-digital occlusal indicators (Fig. 5) (Qadeer et al. 2020; Andrus et al. 2019).
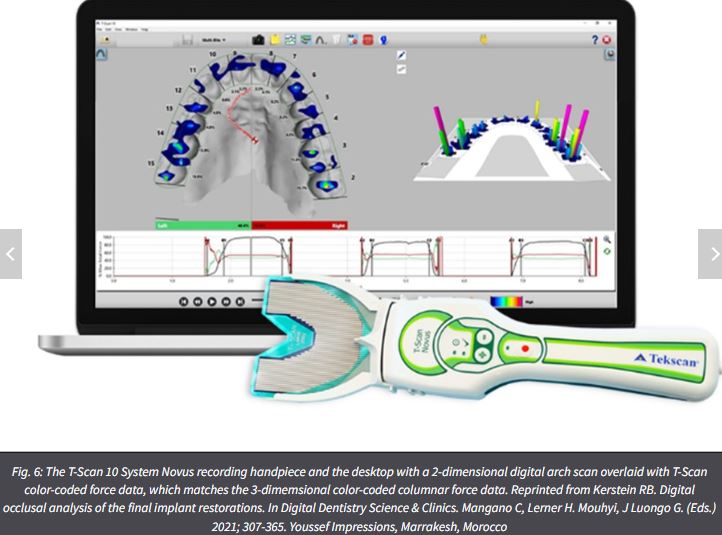
Functional occlusal data sets are recorded intraorally with an ultra-thin, Mylar-encased 100-um thick electronic printed circuit sensor, shaped in the form of a dental arch (Novus HD sensor, Tekscan Inc. S. Norwood, MA, USA) (Figs 6 – 7) that is placed between the patient’s teeth, as they occlude into maximum intercuspation or make lateral excursive movements. The HD sensor sits in the Novus recording handpiece that connects to a computer workstation via a USB interface, and transmits a stream of digital occlusal contact information to the software for presentation to the dentist on the T-Scan 10 desktop.

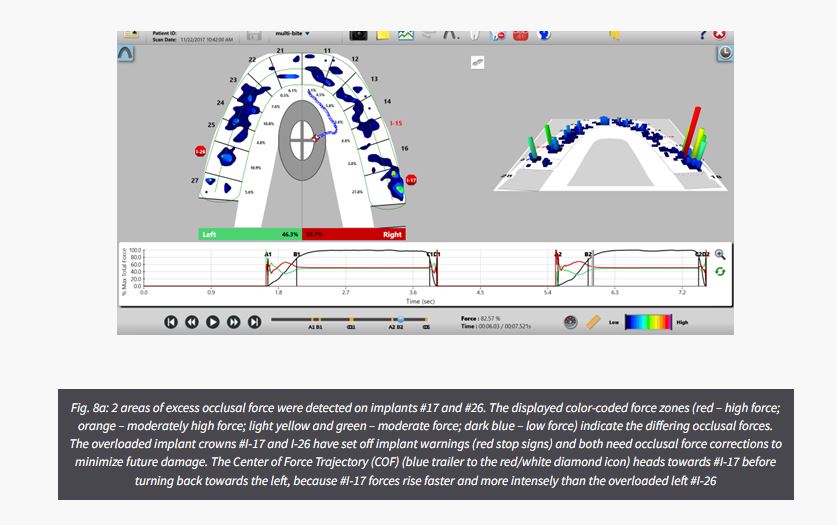
When a patient occludes upon an HD sensor, the opposing teeth make approximating contact that compresses together the upper and lower sensor surfaces, which results in a change in the electrical resistance in each of the compressed 1-mm2 force measurers (the sensors contain between 1500-2200 force measurers). These resistance changes are then measured by the T-Scan’s hardware electronics as a change in digital output voltage (DO). When the contact force applied is higher, it produces larger resistance changes, and lower occlusal contact force produces lesser resistance changes. A map in the T-Scan 10 software receives a stream of changing sensel digital output voltage values (from the recording handpiece) and organizes them in the same orientation the sensels have within the sensor matrix. These contact-induced voltage changes are presented to the implantologist in a multi-colored, 2- and 3-dimensional dynamic video playback graphical display (Fig. 8a) (Kerstein 2020).
The digital indicator system detects whether an occlusal force on one set of contacting opposing teeth or implants is greater, equal to, or less than the occlusal forces occurring on other contacting teeth throughout the dental arches. This aids the implantologist in diagnosing excessively high occlusal force concentrations, while simultaneously diagnosing where there is little, moderate, low, or no occlusal force present in other areas of the same occlusion (Kerstein 2020). Determining where excessive relative forces are concentrated on implant prostheses can accurately diagnose their location for precisely targeted computer-guided time-based and force-based occlusal adjustments.
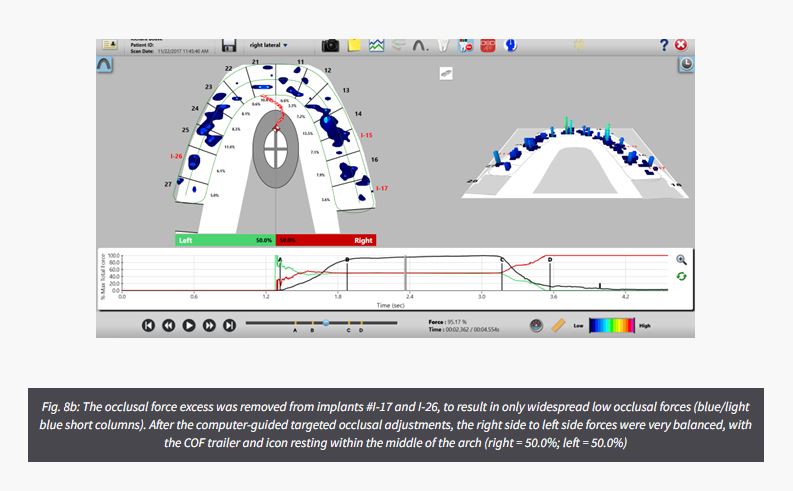
An example of this computer-guided closure into MIP force control that develops improved occlusal force balance in a patient with 3 isolated single implants crowns can be seen in Figures 8a and b. The maxillary 2nd molar implant #I-17 is holding excessive and intense contact forces (32.7% of the entire occlusion), which set off an overloaded implant warning (red stop sign), while also causing the patient significant bite discomfort since this crown was initially placed 2 years prior. Excess occlusal force was also detected on implant #I-26, setting off another overloaded implant warning. By using the T-Scan technology to target these 2 overloaded implant crowns with computer-guided occlusal adjustments, widespread, low force occlusal balance was established that did not raise any implant warnings (Fig. 8b). Then, following closure and balance corrections, excursive lateral and protrusive movements were optimized.
Digital occlusal indicators can increase chair time when performing computer-guided occlusal treatment, because it requires the clinician to meet high-telorance occlusal metrics to measurably establish a low-force and balanced outcome (Fig. 8b). Also, digital sensors do not mark the occlusal contacts which means that an articulating paper is still needed, but only to “mark” contacts. Its appearance is not “judged subjectively” for perceived force content because the digital indicator data targets the specific contacts for adjustment. Another limitation is that these indicators do not measure absolute force in engineering units (Kerstein 2020). Finally, there is a definite learning curve required of clinicians (involving didactic amd clinical training), to develop the chairside skills required for optimal computer-guided diagnostic and treatment effectiveness (Afrashtehfar & Qadeer, 2016).
a) Clinician related advantages
There are many clinical advantages for the clinician when using this technolgy compared to using traditional occlusal indicators (Qadeer, 2020) including:
b) Patient related advantages
There are also a number of patient advantages to T-Scan, as well (Qadeer 2020) that also include:
The deleterious consequences of choosing the wrong contact to adjust occlusion are potentially many, because undetected high force contacts are left in place and eventually cause cyclic overload of an implant prosthesis, while healthy undetected low-force contacts may be inadvertently adjusted away. Contact selection subjectivity certainly plays a definitive role in the high rates of occlusal and implant material complications that occur with dental implant restorations. This is the main reason installing implant prostheses with the objective force and timing metrics of the digital occlusal indicator technology like T-Scan helps aid in both long-term implant component material survival and peri-implant biomechanical health.
Dr. Robert Kerstein is a Clinical Consultant for Tekscan Inc., Norwood MA, USA. He receives no compensation for sales of any Tekscan products
For product information on T-Scan or to purchase click here.
If you would like us to visit your practice and give you a T-Scan Demo, give us your details here and we will be in touch to arrange it.
With permission from Tekscan and ITI (original Blog source)

Over many years, the IPS e.max Press material and the Programat G2 press furnace have been consistently further developed to work together smoothly. The benefits of these fine-tuning efforts are clearly revealed in the fabrication of esthetic anterior restorations. Nicola Pietrobon, a seasoned dental technician, shows the excellent results he is able to achieve with this winning combination.
The restorations presented here were created in collaboration with Dr med. dent. Stefan Paul in Zurich, Switzerland.
Preoperative situation
The patient presented to our laboratory because she wished to have the appearance of her front teeth improved. The enamel defects had previously been built up and enhanced with composite resin. However, the result was not to her satisfaction

Figure 1: The photo shows the preoperative view before the treatment commenced.
Procedure

Figure 2: Nicola Pietrobon uses a Programat EP 5010 G2 to create IPS e.max Press restorations

Figure 3: In the laboratory, the pressed IPS e.max Press crowns and veneers were prepared for their placement in the patient’s mouth.
6. Cementation:
The prepared crowns and veneers were etched in preparation for cementation.

Figure 4: The completed crowns and veneers were placed in the patient's mouth.
The outcome clearly demonstrates how state-of-the-art ceramic materials are capable of reproducing the natural tooth structure and what type of restorations can be produced with them.
The IPS e.max Press restorations were successfully placed, and everyone involved in the case was highly satisfied with the result. Due to their true-to-nature translucency and opacity* the ceramic restorations blended in seamlessly with the natural teeth. The outcome clearly demonstrates how state-of-the-art ceramic materials are capable of reproducing the natural tooth structure and what type of restorations can be produced with them.
Better trust the original: the Ivoclar press technology. Lab-proven. Future-proof.
Original source Ivoclar Blog - posted with permission

With his key interest in Digital Aesthetic Dentistry and Implantology, Dr Waldo Engelbrecht from Enamel Clinic in Cape Town uses Tekscan’s T-Scan - dentistry’s premium digital occlusal analysis system. He told IVOblog it’s something he now uses every single day.
“T-Scan has really improved a number of steps when I am treating patients.
The diagnostic value is really amazing, especially for patients who have discomfort but cannot pinpoint it and we as clinicians cannot see where the problem lies. I’ll use the T-Scan and see that there actually is an interference that we can adjust.
Even patients with sensitive teeth can start to be treated by removing the heavy contacts.
It is also great for checking occlusion after placement of crowns, bridges and implant crowns. It makes a lot more sense than when you just use normal bite paper because you can identify where the heavy contacts are and which aren’t problem areas.
This saves a lot of time as it eliminates having to conduct multiple, repetitive follow-ups– you can get to the cause of the problem much quicker.”
Located in the Innovation District of Boston, Tekscan has been in business since 1987. T-Scan™ provides dynamic occlusal measurement - revealing the level and timing of force on individual teeth and the occlusal stability of the overall bite. Nearly EVERY dental procedure performed impacts occlusion. Poor occlusion affects quality of life. T-Scan is a tool used by dentists to restore this quality of life. Click here to view Tekscan products on IvodentOnline.




