
Fresh Breath Month has traditionally focused on managing bad breath through microbial control and hygiene-based interventions. In 2026, it presents an opportunity for the oral healthcare industry to elevate the conversation, shifting from short-term fixes to biologically sound, ethically responsible approaches that support long-term oral and systemic health.
For dentists, oral hygienists, educators and industry partners, Fresh Breath Month should serve as a platform to promote best practice, clinical credibility and evidence-based decision-making, grounded in an evolving understanding of the oral microbiome.
From eradication to equilibrium
The historic approach to fresh breath has often centred on antimicrobial “kill-all” strategies and odour masking. While these may provide temporary results, emerging research confirms that indiscriminate bacterial removal can disrupt the oral ecosystem, delay healthy recolonisation and favour opportunistic pathogens.
The modern paradigm reframes fresh breath as a function of:
The key insight is clear: removing what matters is about disrupting the harmful ecosystem, not sterilising the mouth.
Fresh breath is therefore not about eliminating bacteria, but about cultivating a healthy, resilient oral microbiome.

Why microbiome preservation matters
The oral microbiome performs essential biological functions that extend well beyond breath quality. These include:
As a highly adaptive and context-dependent system, the oral microbiome relies on balance. Broad antimicrobial approaches risk removing beneficial species, impairing recovery and contributing to dysbiosis, with implications for periodontal health, bad breath recurrence and systemic inflammation.
Clinically responsible care therefore prioritises selective disruption of pathogenic biofilm while preserving structurally and biologically valuable tissues and microbial communities.
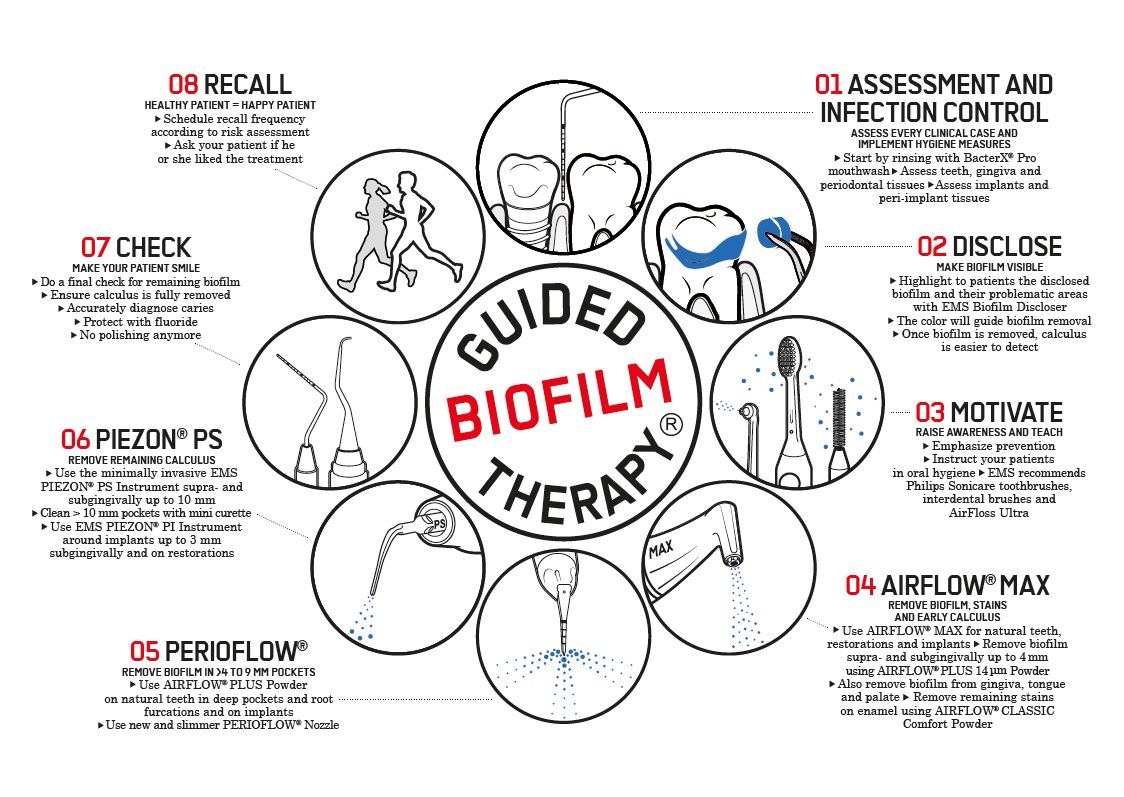
The role of Guided Biofilm Therapy (GBT)
EMS Guided Biofilm Therapy (GBT) exemplifies this biologically aligned approach. Built on the principle of “remove what is biologically harmful, preserve what is structurally and biologically valuable,” GBT supports ecological biofilm management rather than aggressive debridement.
GBT is particularly relevant in the context of fresh breath management because:
Clinically, GBT has been shown to improve immediate breath quality, enhance patient perception of cleanliness and comfort, and support higher compliance with ongoing preventive care.
Alignment with modern dental principles
Within a Fresh Breath Month framework, GBT aligns strongly with:
By supporting microbial balance rather than disruption, GBT reflects the future direction of evidence-based dentistry.

Factors that influence oral microbial balance
Professional care must be supported by informed patient behaviour. A healthy oral microbiome is influenced by the following factors:
These behaviours empower patients to support long-term oral and systemic health.
Looking ahead
As research continues to deepen our understanding of the oral microbiome’s role in inflammation, cardiovascular health and systemic wellbeing, the message for Fresh Breath Month is clear: the future of dentistry is not about doing more, it’s about doing what matters, better.
Fresh breath is not a cosmetic endpoint. It is a clinical indicator of balance, health and responsible care.
From #ChairToCare, this is how long-term oral health is built.

The Fresh Breath Insights 2025 survey, conducted by Ivodent in partnership with GUM, gathered insights from 170 South African dental professionals - including general dentists, specialists, oral hygienists, dental assistants and technicians. It highlights a pressing need for more patient education and increased awareness.
We sincerely thank everyone who contributed their expertise to help clarify the oral health landscape in South Africa.
How Common is Bad Breath?
We all know bad breath is a widespread issue. The survey found that:
Why Don’t People Talk About It?
Despite the high prevalence of bad breath, it remains a sensitive subject. While 82% of dental professionals said they feel comfortable discussing halitosis, there are still barriers. According to the survey:
Leading Causes of Bad Breath
The survey confirms that poor oral hygiene is the primary cause of bad breath in South Africa.
Do you agree with these leading factors?
Additional factors mentioned included fasting, mouth breathing, and alcohol-based mouthwashes.
Poverty is another issue, with some patients unable to afford basic oral care products. “Clients are often unable to afford something as basic as toothpaste, toothbrushes, or mouth rinse,” said one respondent, reinforcing the need for affordable, accessible solutions and more education on cost-effective oral hygiene.
Dental Professional-Approved Solutions for Fresh Breath
As dental professionals, you know that the most effective solutions for bad breath are rooted in daily oral hygiene. The top solutions, according to the survey, include:
Additional solutions include addressing dry mouth (xerostomia) and advising patients to avoid smoking and alcohol-based mouthwashes, both of which exacerbate the issue.
Fresh Breath Month: Educate Your Patients
With Fresh Breath Month in February, now is the perfect time to educate your patients on the causes of bad breath and its solutions. As dental professionals, you are ideally positioned to guide your patients in making simple, lasting changes to improve their oral health.
Encourage them to take the online Bad Breath Check to assess their breath.
By promoting effective at-home oral hygiene, we can empower patients to take control of their oral health for fresh, beautiful smiles.
Key Takeaways
Bad breath doesn’t have to be embarrassing or neglected. By addressing the root causes and giving expert advice, you can help your patients achieve fresh breath.
We’d love to help! Chat with your Ivodent rep about GUM’s trusted oral care solutions.
Survey notes:
Ivodent conducted the Fresh Breath Insights 2025 Survey with GUM, the global oral care brand. The survey was distributed online via email and social media, including through the South African Dental Association’s (SADA) platforms. With 170 respondents from across the dental industry, this survey provides essential insights into the state of bad breath management in South Africa.
Thank you once again to all the dental professionals who participated. Your input is invaluable. Let’s continue to work together to improve patient care and provide the educational information and solutions patients need.

IVOblog Quick Q&A recently asked Dr Redelinghuys, a dentist in Pretoria (who specialises in Root Canals), what she loved most about her new Ivoclar CS6 combination furnace: her Quick answer! “Having a patient “all done in a day!”
Q: Has the Ivoclar CS6 combination furnace made one day visits for your patients easier?
I love the super fast crystallisation and sintering for both Zirconia and e.max. Even with Zirconia I can do a patient in one sitting which is great for some patients that struggle to find the time to come to the dentist. And of course with e.max it’s so much easier to do a one-day visit for a patient even with multiple teeth. Patients really like the one day visit - only one set of injections for one appointment! They may wait a while as we work, but it can all be done in a day!
Q: Have you noticed that your zirconia crowns have better translucency due to the Vacuum assisted sintering technology.
I am most excited for Crowns, this is the first sintering oven we have had and I am so impressed with the aesthetics – you can really see the difference!
Q: The fact that you can sinter a 3Y type LT Zirconia in 22 minutes must be a massive game changer for you.
Yes, its amazing to be able to do LT Zirconia for 7's and 6's, especially for patients that grind. It’s fantastic where minimum thickness is a problem. And sintering is super fast!
Q: How do you find the aesthetics of the MT MULTI Zirconia.
I am very happy with the MT Multi Zirconia – it blends well with the natural teeth right next door. I have done a few 3-unit bridges and got a very nice blend between the natural teeth and the Zirconia – you can’t see the difference. I have also done a 4-unit bridge.

The MDP-based adhesive functional monomer found in various Ivoclar products has been specially formulated to ensure high bond strengths to various substrates.
MDP consists of a long-chain methacrylate with a phosphoric acid group.
The phosphoric acid group enables a stable chemical bond to zirconium oxide and base metal alloys. Consequently, using an additional bonding agent or primer is not required for permanent bonding to these restoration substrates.
In addition, phosphoric acid reacts with the calcium ions of the dental hard tissues and, in the process, produces a bond with the tooth structure. The need for a separate adhesive is eliminated.
Which Ivoclar products contain 10MDP?
1. Tetric N-Bond Universal – The Universal adhesive for bonding direct and indirect restorations. The acidic monomer MDP bonds to the calcium within the hydroxy apatite to form insoluble calcium salts, facilitating mechanical blockage and sealing in the dentin tubules. This helps prevent the movement of fluid in the dentin as well as post-operative sensitivity associated with that movement.

2. Monobond N – The universal primer for conditioning of all indirect restorations. The acid monomer MDP improves bond strength to zirconia and metal surfaces. The MDP bonds to zirconia on its free phosphate group and to resin cements on its methacrylate end.
Monobond N is distinguished by an innovative combination of three different functional adhesive monomers: phosphoric acid methacrylate, silane methacrylate and sulfide methacrylate. This combination enables the universal primer to bond to zirconia, glass-ceramics and metal alloys.

3. Multilink Speed - A clinically proven self-adhesive resin cement with MDP within its formulation for the permanent seating of high-strength restorations made of zirconia and metal, both on natural teeth and implant abutments. Given its self-curing, self-adhesive properties, Multilink Speed offers peace of mind and security, especially when cementing opaque restorations.

Zirconia (zirconium oxide)-based ceramics have become a very popular type of all-ceramic restorations. Zirconia-based ceramics have a high strength and, therefore, restorations can be cemented with traditional cements or bonded with resin cements.
Zirconia crowns and bridges with adequate thickness, good retention and fit, do not need bonding (do not rely on high bond strengths) and can be cemented with conventional cements.
If greater retention to tooth structure with minimal marginal leakage is required, bonded cementation with resin cements is recommended. Adhesion to tooth structure and to the ceramic restoration combines good marginal sealing and strengthening of the tooth-restoration complex to minimize marginal leakage and tooth fractures.
Conventional cementation with glass-ionomer cement (GIC), resin-modified glass-ionomer cement (RMGIC) or self-adhesive resin cement - If your cement does not contain the MDP (as in the case with GICs, RMGIs, some self-adhesive resin cements and all adhesive resin cements), a MDP primer needs to be applied to the fitting surface of the restoration.
If your cement already contains MDP within its formulation (as in the case with Multilink Speed), a MDP primer is not required on the fitting surface of your restoration.
Self-adhesive resin cements are the best choice for zirconia-based ceramic restorations, when the restoration does not require the highest retention.
Self-adhesive resin cements are less technique sensitive than bonding with adhesive resin cements and offer more retention and better marginal sealing of tooth structure than the traditional glass ionomer cements. No separate bonding agent is necessary, reducing much time and effort, and cleanup is easy with self-adhesive resin cements.
When more retention is needed due to a short clinical crown or an over tapered preparation, adhesive resin cements, may be used to bond the restoration. Adhesive resin cements do not contain MDP within its formulation and therefore a primer to the restoration surface and a bonding agent is to be applied to the tooth surface.
Zirconia cementation with Multilink Speed – your self-adhesive resin cement:
Air-particle abrasion (sandblasting) of the zirconia restoration before cementation - 30-60ų alumina particles for 5 seconds. This is done by your dental laboratory after fabrication of the restoration.
1. CLEANING: During try-in the restoration becomes contaminated with phospholipids, saliva and blood. The intaglio of the crown therefor has to be cleaned with a special ceramic cleaner after try-in. Ivoclean is the universal extra-oral cleaning agent for the decontamination of the fitting surfaces of restorations after try-in.
2. APPLY CEMENT: Apply cement into restoration and seat on tooth. No zirconia primer is required when using Multilink Speed, as it already contains the acidic monomer MDP within the cement formulation. No bonding agent is required on the tooth surface as the acidic monomer MDP within the cement formulation bonds to the calcium within the hydroxy apatite to form insoluble calcium salts facilitating mechanical blockage and sealing in the dentin tubules.
Zirconia cementation with Variolink Esthetic DC – your dual curing esthetic adhesive resin cement:
Air-particle abrasion (sandblasting) of the zirconia restoration before cementation - 30-60ų alumina particles for 5 seconds. This is done by your dental laboratory after fabrication of the restoration.
1. CLEANING: During try-in the restoration becomes contaminated with phospholipids, saliva and blood. The intaglio of the crown therefor has to be cleaned with a special ceramic cleaner after try-in. Ivoclean the universal extra-oral cleaning paste for the decontamination of the fitting surfaces of restorations after try-in.
2. CERAMIC PRIMER: The adhesive resin cement Variolink Esthetic does not contain the acid monomer MDP within its formulation and therefor a ceramic primer containing MDP needs to be applied to the fitting surface of your restoration. Monobond N the universal ceramic primer with MDP is used.
3. TOOTH SURFACE: All adhesive resin cements require the tooth surface to be bonded with a separate bonding agent. Tetric N-Bond Universal is used on the tooth surface, dispersed with air and cured.
4. APPLY CEMENT: Apply Variolink Esthetic DC resin cement into restoration and seat on tooth.

Dr. Giuseppe Chiodera, an honorary member of Style Italiano, loves developing new treatment techniques that simplify diagnostic and restorative procedures.
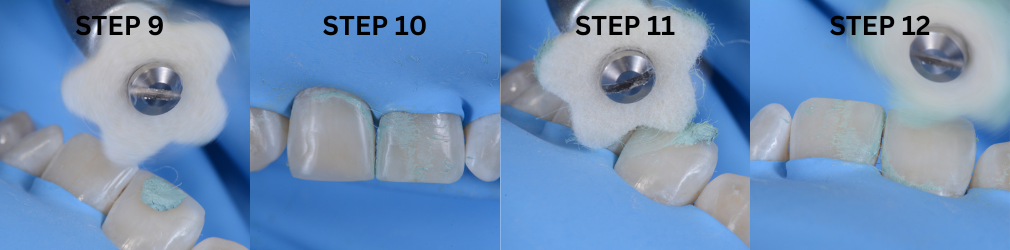
Lucida Paste a sub-micron hybrid water-soluble patented polishing compound for extreme gloss in combination with the felts.
For more product information click here.


Clinical Management of Deep Subgingival Margin Elevation in Posterior Teeth with Structural Compromise.
The understanding of restorative dentistry today demands not only considering the preservation of remaining tissues but also respecting the biomechanics governing the dental structures, having as main objectives the preservation of pulpal health and strengthening fragile and more affected teeth, providing a clinical treatment with the longest possible lifespan.
Within routine clinical practice, restorative concepts and techniques aim to bioemulate lost tissues in terms of structure and function. Precisely one of the most demanded techniques today for our indirect restorative procedures is the relocation of cervical margins or deep margin elevation. This clinical approach was first described in 1998 by Dietschi and Spreafico, who defined it as "a technique indicated in cases with slightly subgingival margins, where it is possible to relocate the cervical area of a preparation more coronally by applying appropriate increments of composite resin on the existing margin. This procedure should be developed under absolute isolation with a rubber dam, followed by the placement of a metal matrix band" (1). Since the introduction of this new concept, other authors and publications have emerged, emulating the technique, and applying it to various scenarios in restorative dentistry. In terms of posterior indirect partial restorations, elevating the cervical margin of a preparation above the gingival margin provides advantages for impression taking and subsequent isolation during the cementation process. However, fundamental requirements must be taken into consideration in order to ensure a correct adhesive procedure: complete isolation of the cervical margin of the preparation and placement of a matrix band that achieves perfect sealing of the cervical area. Otherwise, the technique is contraindicated.
Once the technique is performed, a bitewing radiograph should be taken to evaluate the adaptation of the composite resin in the gingival area, checking for gaps or over-contours before proceeding with the final impression (2).
In terms of clinical elements to consider for correct clinical performance, a curved matrix is recommended to ensure not only perfect sealing in the gingival area but also the formation of a correct emergence profile. In this situation, the use of ReelMatrix™ margin elevation bands from Garrison (Fig. 1) is recommended. Due to their thickness, contour, and height, these bands achieve anatomical margin elevation in most cases. Like other bands designed by the same company, they have two different surfaces: one coated with Teflon to improve handling of the restorative material and another with a rigid metallic surface. This band, which was specially designed for this technique, should be attached using a tensioning instrument (Fig. 2) which places this band on the cervical margin of the preparation with efficiency and precision.
Clinical Case
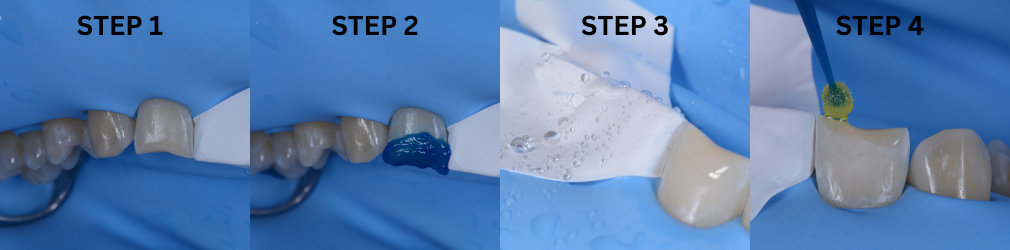
A 20-year-old female patient visits the dental clinic due to moderate pain and expresses a desire to replace an old restoration. Upon clinical examination, a composite resin restoration partially covering the occlusal surface of tooth 2.4 is observed, showing marginal gaps, secondary caries, and deficient anatomy (Fig. 3). Based on the specific structural diagnosis, an indirect composite resin restoration on a stress-controlled biobase was indicated. This will maximize adhesive strength through a rigorous biomimetic restorative protocol associated with deep margin elevation in the mesial proximal box without the need for prior surgical intervention.
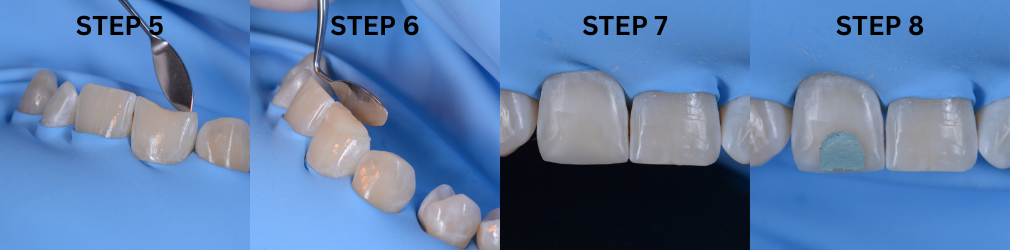
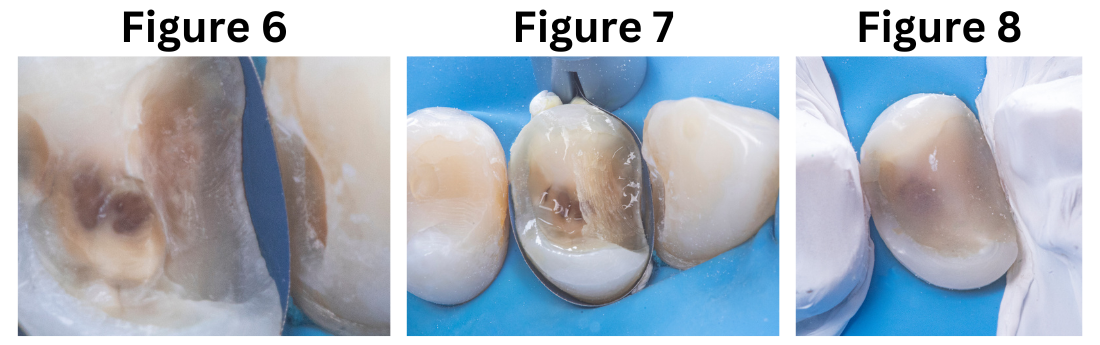
The procedure described above was performed in two phases. The first phase focused on primarily replacing the dentin, for which the old restoration was completely removed (Fig. 4). Subsequently, the tensor-band complex was placed to elevate the cervical margin using the ReelMatrix™ Deep margin Elevation system (Fig. 5). The image shows the band's adaptation to the tooth, achieving a perfect marginal seal (Fig. 6). Immediately after, the adhesive phase was complete, followed by the application of a hydrophobic layer of Flow and finally a 3mm strip of polyethylene fiber to ensure adhesion, along with a thin layer of (Fig. 7). Subsequently, layers of composite resin, not exceeding 1mm in thickness, were applied to achieve progressive buildup. Once the biobase was established, a minimal biological preparation was performed using diamond burs, and a definitive impression was taken for the fabrication of the indirect restoration (Fig. 8).
In the second phase, under absolute isolation, the indirect restoration was connected to the previously constructed biobase using an adhesive bonding agent, to ensure high mechanical properties and favorable aesthetics. Excess material was carefully removed, mainly in proximal areas, and after curing, the rubber dam was removed for the final view of the restoration, evaluating harmony with the periodontal tissue and occlusion (Fig. 9+10).



References
Bio for Dr. Patricio Gutiérrez:
Dr. Gutierrez is a graduate of the dental school of the Pedro de Valdivia University, in Santiago, Chile.
He has carried out his entire career in the private sector, in different private clinics located in Santiago.
Since he got his degree, Dr. Gutierrez has trained and practiced restorative and aesthetic dentistry, this being his area of interest. In 2016, he participated in the aesthetics diploma in adhesive oral rehabilitation at the dental school of the University of Los Andes, in Santiago. After that, he held teaching positions at universities and institutes contributing to numerous publications and clinical cases. This vocation led him to obtain a Magister in Higher Education at the Andres Bello University.
Currently, Dr. Gutierrez is studying towards a Diploma in Restorative Dentistry Biomimicry at Diego Portales University, also in the same city Santiago.
Over the past couple of years, Dr Gutierrez, has dedicated himself exclusively to this area, becoming an "opinion leader" of different commercial dental brands that are established in Chile.
View product on IvodentOnline here.



