
Master dental technician Claus Fiderer is specializing in implant prosthetics in his laboratory. As a dedicated user of Ivoclar products, he entered the 2021 prize draw held to celebrate the 30-year anniversary of the press technology. He was lucky and won the first prize: a special gold edition Programat EP 5010 G2 press furnace. In the interview below, he tells us why he enjoys using the press technique and what advantages he sees in using it.
How did you get into dental technology and what do you like about it?
Claus Fiderer: As a child, I used to love building stuff, especially model aircrafts. I was fascinated by the precision mechanics behind these things, and I still am. My dad was a dentist and so there was a connection with dentistry from an early age. One thing led to another and I decided to go into dental technology. I especially enjoy that part of my work that requires high precision and fine detail.
What services do you offer in your laboratory?
Claus Fiderer: We specialize in implant-supported and telescopic dental prostheses. It is essential for us to collaborate closely and smoothly with our dentist customers. We see ourselves as a service provider that always strives to achieve the best possible result. We care greatly about providing in-depth advice and that is why we like it when patients come to see us in person in our laboratory. This way, we have the opportunity to assess our long-term results, once the patients come back a few years down the line. This is what makes our work exciting and gives as a lot of variety in what we do. What pleases us most is when patients tell us how happy they are with their restorations.
What are your motivations behind using press technology and especially lithium disilicate press ceramics (IPS e.max Press) from Ivoclar?
Claus Fiderer: Up to around 1997, we did all sorts - layering on dies and what not. Then came along Ivoclar’s lithium disilicate press ceramics: IPS Empress. The first of its kind so to speak. All of a sudden there were many more possibilities available to us than just layering. My decision was also motivated by the fact that restorations became a great deal more profitable with the press technology. Ivoclar must clearly be seen as the pioneer of the press technology. Over the years, I would never have wanted to use anything else, true to the motto “never change a winning team”. Why would I want to replace something that works so perfectly well?
The service also deserves a mention here: There is always a contact person available in the unlikely event that something does not quite work the way it should. That’s really important to me and simply has to be in place.
Do you already own a press furnace from Ivoclar? If yes, which features do you particularly like about it?
Claus Fiderer: The old Programat furnace (EP 3000) that we have been using in our laboratory has always served us well. We didn’t think of replacing it. The prize draw, however, has given us the opportunity to do that and we are absolutely delighted with the new press furnace. We have always loved our old furnace because it has always worked. It is intuitive to use and we were always able to achieve reliable and consistent results. Simply a very reliable piece of equipment.
What advice would you give to other dental technicians who are not yet using press technology?
Claus Fiderer: Start using it tomorrow – or better still, start using it today! Why? Press technology offers many more possibilities, especially in the anterior region. This is exactly where press technology has become indispensable. And not only that, but the selection of different press ingots allows you to achieve custom-tailored restorations really quickly and easily.
I trust IPS e.max Press because …
Claus Fiderer: … there is no substitute for Ivoclar’s many years of experience.
Visit our IVODeals page to see our deal on IPS e.max Press

Original source Ivoclar Blog - posted with permission


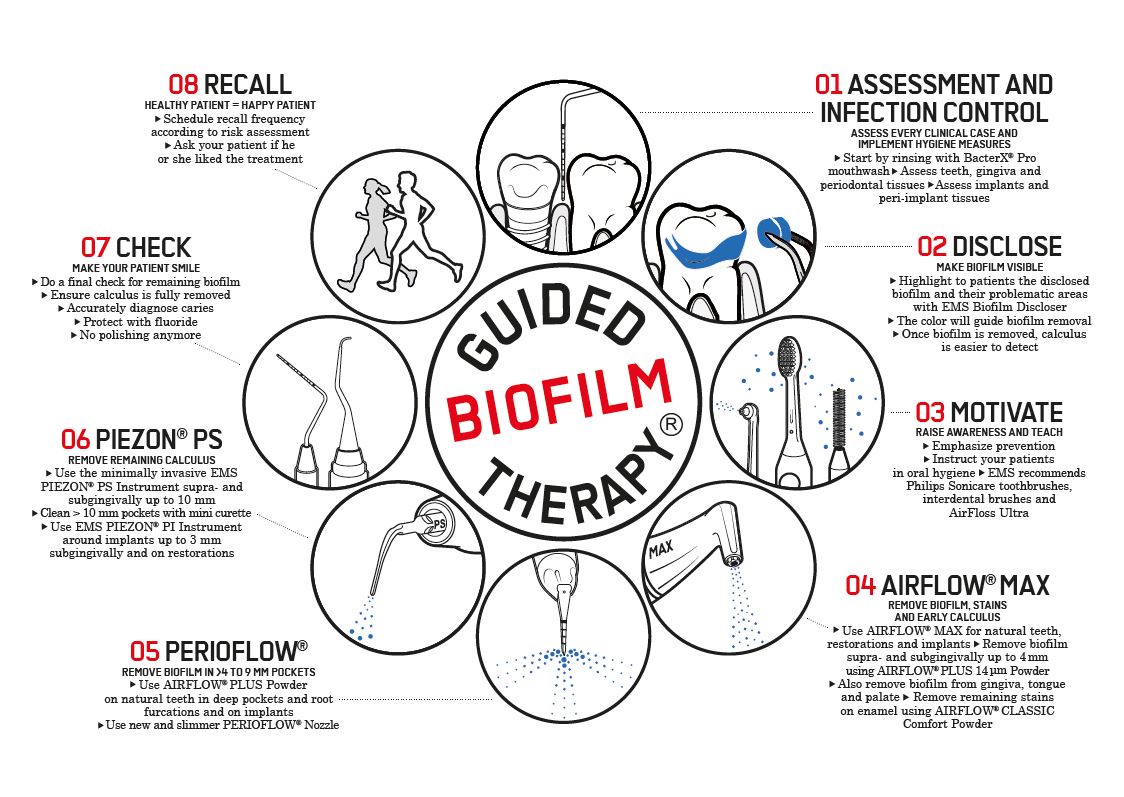
Are you GBT Certified yet?
Does your team and your practice meet the GBT Certification requirements?
Here’s the Checklist to find out:
A practice must have the following in place to qualify as “GBT (Guided Biofilm Therapy) Certified” and to get all the benefits:
1) Own a premium GBT device – either the EMS AirFlow Prophylaxis Master or AirFlow Master Piezon to perform full Guided Biofilm Therapy.
2) Professionals using these devices must be Swiss Dental Academy (SDA) trained and follow the 8-step GBT Protocol (training needs to be updated every two years).
Training includes a 4-module on-demand online course (based on the latest scientific research) on all the aspects of GBT (x11 CPDs). It uses both a multi-functional, interactive learning programme hosted on the Ivodent eCademy, followed by an in-person training session (x8 CPDs) by an SDA accredited trainer.
Cost: R1 200 (incl VAT) for both the 4-module online on-demand and also the in-person training – for a total of x19 CPD points.
GBT Certified practices also have access to paid-for and free e-learning updates and webinars, keeping up to date with all the latest research, technologies and clinical practice standards.
All existing GBT qualified practitioners who have completed an SDA course with Ivodent on or before 30 July 2022, will get access to the 4-module course at no cost, to update their training, and earn x11 CPD points. The in-person session is not needed. The GBT training is valid for two years. All professionals that completed the SDA GBT course before 2019 must complete the online modules within 6 months to stay GBT qualified.
3) Use exclusively original EMS products, EMS Swiss Instruments and EMS Airflow Powder.
4) Agree to uphold the GBT Consensus confirming evidence based clinical efficacy.
5) Complete and submit x10 patient surveys to EMS (additional x40 over 6mths after certification).
Every GBT certified practice is given a Swiss Dental Academy (SDA) plaque and a framed GBT Certificate to display at their premises. They are also offered marketing support by EMS and will have access to GBT marketing materials and patient fliers to promote GBT and their VIP status to patients, as well as copy and paste social media templates, GBT pictures and logos for their website. All GBT certified practices are added to consumer location finders on both Ivohealth and the EMS global website.
The SDA approved GBT on-demand and in-person course will be included, free of charge, when you purchase a Premium EMS device.
Already attended the course and purchasing a premium device? You will be credited with R1 200 worth of materials to reimburse the cost of course fees paid.
Book your on-demand course today and receive consumables to the value of R1 200 if you decide to proceed.
Contact your local Ivodent rep or email Stephanie Burgess on [email protected] to book your free EMS demo or for further details on how to become part of an exclusive global network of passionate dental professionals, performing dental prophylaxis at the highest possible level.
Visit the Ivodent eCademy for details on GBT courses, course payment and access.

Uncompromisingly Natural Oral Care – Now With Probiotics and Prebiotics
Introducing Olgani Probiom, South Africa’s first toothpaste and tooth powder formulated with probiotics, for a healthy oral microbiome and total wellness.
The new Olgani Probiom range is the latest innovation from Olgani Naturals, manufacturers of ‘uncompromisingly natural’, premium oral care. The all-natural toothpaste and tooth powder contain live probiotics, prebiotics and a carefully selected range of active, edible ingredients for a healthy mouth and body.
Why Put Probiotics in Oral Care?
The mouth is the beginning of the digestive tract and is home to more than 700 bacteria, viruses and fungi; it is the body’s second most abundant microbiome, after the gut. When in balance, this ecosystem works in harmony. An imbalance can cause oral disease, including cavities and gum disease, and also spread to other parts of the body, contributing to chronic disease.
Probiotics are ‘good’ bacteria with well-known health benefits for the immune system and digestion. Research over the past decade has demonstrated their oral health benefits – helping prevent cavities, gum disease, fungal infections and bad breath (aka halitosis). People with healthy teeth and gums have been shown to have a robust, balanced oral microbiota.
Olgani Probiom contains two probiotics – Lactobacillus rhamnosus and Lactobacillus casei – which have been shown to have significant oral health benefits
Prebiotics are insoluble fibres that feed probiotics. Olgani Probiom contains Olgani’s signature Prebio+ care blend of prebiotics, with inulin and xanthan gum, to help maintain and nourish a healthy microbial balance.
Olga Niemkiewicz, founder and managing director of Olgani said the new Probiom range was developed after months of research and testing. “It is well-documented that your microbiota influences the entire body’s functioning. Microorganisms in your mouth are directly connected to your gut. It makes sense to try to balance and support oral microbiota in support of complete wellness.
“We selected the ingredients in Probiom to fortify and nourish the microbiota in the mouth. Prebiotics and probiotics help to increase the number of friendly bacteria. Herbal extracts and mineral clays support healthy gum tissue and provide vital minerals to support the remineralisation of enamel and to protect dentine.”
Active, Natural Ingredients
The nourishing ingredients in Olgani Probiom include detoxifying bentonite; nutrient-rich chlorella; French green clay; green tea; antibacterial, antioxidant and anti-inflammatory lemongrass; refreshing peppermint as well as probiotics Lactobacillus rhamnosus and Lactobacillus casei and prebiotics inulin and xanthan gum.
Olgani Probiom does not contain fluoride, sodium lauryl sulphate (SLS) or other foaming agents, glycerine, sorbitol or sweeteners, titanium dioxide or any artificial preservatives, taste enhancers or additives. It is vegan and cruelty-free.
The tooth powder comes in zero-waste packaging – a biodegradable box, glass jar and aluminium lid – and, because its production requires less water and electricity, is an extremely environmentally-friendly oral care option.
Testimonials
Wellness doctor and integrative health practitioner, Dr James Liddell said that the probiotics in Olgani Probiom will help repopulate the mouth with healthy bacteria which can reduce bad breath, cavities and periodontal disease. He likes the fact that Probiom is free from controversial ingredients like sodium lauryl sulphate, fluoride and triclosan. “Olgani Probiom has a wide range of oral health benefits and leaves the mouth feeling fresh and clean. I love the lemongrass and peppermint flavour.”
Dentist Dr Marieke Fraenkel described Olgani Probiom as ground-breaking and said she enjoyed the fresh taste.“I finally have an answer to promote a healthy oral microbiome to my patients, diminishes sensitivity, an answer to halitosis and assistance to the gut biome to support holistic health without polluting your body or the planet.”


Is light polymerization a necessary evil or just a short, intermediate step? The Canadian dental clinician and researcher Richard Price at Dalhousie University in Halifax has spent the better part of the past few decades studying curing light technology. In an interview with Dental Tribune he shared his advice on how to light cure properly and explained why polymerization lights are so important for the success of your dental office.
Dr. Price, you have been instrumental in researching curing light technologies. Would you mind sharing your thoughts about compromised polymerization and its potential effects on clinical success?
Thank you for this opportunity to discuss the importance of using a good curing light to prevent undercuring dental resins. The problem as I see it is that most dentists were never taught much about the importance of proper light curing, or what to look for in a good curing light. Even the cheapest light and the sloppiest technique will produce a resin restoration that is hard to touch with an explorer. The problem is that the dentist cannot determine whether the bottom or the inside of the composite restoration has been adequately cured. An under-cured restoration is weaker and more prone to fracture, the bond strength to the tooth is reduced or even non-existent, post-operative sensitivity occurs, the color stability of the resin is compromised, and more chemicals are released into the body from the partially cured resin. These are all very undesirable outcomes of inadequate light curing, and none of them need to occur.
What should dental professionals consider key attributes of curing lights?
Curing lights are defined as medical devices and only approved medical devices should be used on patients. If we look at Ivoclar Vivadent’s curing lights, they are not only approved medical devices, but they are also functional, ergonomic, reliable, and thoroughly tested according to international standards. Furthermore, the broad emission spectrum of Bluephase lights means that they will cure all known dental resins and bonding systems.
Which key attributes of the Bluephase PowerCure will clinicians find helpful?
In addition to the new Polyvision technology, the light's high power and irradiance can cure both direct and indirect resin restorations. Depending on the thickness of the indirect restoration, the light can photocure the resin cement used to bond most indirect restorations to the tooth. I like to use several exposures using the Turbo or the 3s settings to photopolymerize the resin under my indirect restorations and the regular high output settings for my direct resin restorations.
The patented Polyvision technology has been described as an inbuilt personal polymerization assistant. How does it work?
The Polyvision feature should help clinicians achieve reliable curing results by automatically detecting if the light tip moves away from the tooth when the curing light is on. Polyvision alerts the operator using vibration or an acoustic signal if it detects movement. Then, depending on how far the light tip moves away from the tooth, it will automatically increase or even stop the light-curing cycle.

Your research shows the importance of uniform beam profile and irradiance. Why is this an important factor to consider?
Ivoclar Vivadent recognizes that the success of its resin-based products depends on them being adequately light cured. Suppose the curing light delivers hot spots of high irradiance and regions of low irradiance. In that case, the composite will not be uniformly and evenly cured. It is like baking a cake in an oven that does not provide even heating. The cake cooks, but not evenly. The current range of Bluephase lights delivers an exceptionally uniform light output and uniform irradiance across the light tip so that the composite is evenly cured.
Should dentists regularly measure the light output from their curing lights, and is a built-in radiometer helpful?
Manufacturers will often sell their light based on a claim that it delivers a high irradiance. The light may indeed deliver a high irradiance, but the power output from the light may be rather low. So how can a high irradiance light also be a low power light?
The reason is how the international standards report the irradiance from the light. In the standard, the total power from the light is first measured. This power is then divided by the area of the light tip to provide the irradiance. This means that to deliver the same irradiance, a light with a 7 mm diameter light tip need only produce half the power of a light with a 10 mm diameter light tip (because the area of a 7 mm diameter tip is half that of a 10 mm tip). In addition, this method provides a single irradiance value that is only an averaged value across the tip; however, because many lights have a poor beam profile, there are often hot spots of high irradiance and areas where the irradiance is rather low across the light tip. I see this all the time in budget lights, and this is completely missed in the international standard that only reports a single averaged irradiance value.
Certain models of Bluephase lights also include a radiometer in the charging base. This integrated tester makes it easy to test the light every day. I know that may seem unnecessary to some, but if you only test your light once a week or once a month, what will you do when the light fails the test, because it will fail at some point? Are you going to recall and redo, at no cost, all the restorations you placed since the last successful test? The solution is to test the light every day, and Ivoclar Vivadent makes this an easy thing to do.
Can you please advise on the correct polymerization technique for dental professionals?
When light-curing, I recommend the following steps:
Do you have any other tips to consider during polymerization that will help clinicians in their light-curing?
For Class II situations, I also cure from the buccal and lingual aspects after removing the matrix band.
I use the same technique for indirect restorations, but I usually use a tacking tip first, clean up the excess cement and then light cure with the tip in contact with the indirect restoration.
Only disinfect the light using the manufacturer’s recommended disinfectant. Some disinfectants can damage the light. Read the instructions to find out what you can safely use on the light.
Check that the end of the curing light tip is clean and has no chips, cracks, or cured resin on it. Using a barrier over the light helps with infection control and prevents resins from bonding to the light. However, when there is an infection control barrier over the light tip of the Bluephase PowerCure, and G4 light, the best option is to use two hands and make sure that the light tip covers the restoration. Watch what you are doing with that light tip.
By Dr Jennifer Bell

One of the biggest challenges with completing clear aligner tooth movement predictably is accomplishing enough interproximal reduction (IPR) on schedule to allow for ideal tooth movement. Many clear aligner cases call for IPR to be accomplished to best level and align teeth. I tend to prefer buccal expansion wherever possible to not only allow for better alignment of teeth but to also allow for improved tongue positioning, reduced buccal corridors, and more ideal occlusal forces on posterior teeth. While buccal expansion has many advantages for patients and continues to be my preference, many cases still require some IPR for best completion. Since IPR is an unavoidable part of orthodontic therapy, it is important to find a more predictable protocol to achieve these results.
When IPR is done well and accurately, tooth movement is more likely to move on schedule and the case is likely to complete on time with fewer numbers of refinements (additional series of trays) required. Profitable clear aligner tooth movement begins with implementing systems that work for reducing the number of visits required or additional aligners needed to complete the case. For my clear aligner patients, I have found a very predictable process using both Garrison IPR hand files and Strauss Diamond rotary IPR discs.
Our patient featured in this article presented with a chief concern of improving the esthetics of her smile and reducing her overbite and overjet for more ideal anterior tooth placement. She has a posterior implant which constricts the amount of buccal expansion we can accomplish so in this particular case, we elected to add some IPR to accomplish her tooth movements. As shown in Fig 1, she had some existing space (green boxes) on the left pre-operative image and required IPR (gray diamonds) in right ClinCheck image to improve midline and position of anterior teeth. Upon delivery of clear aligners to the patient, we will try to complete all necessary IPR at the initial appointment. Of course, there are times when it is more ideal to wait for some movement first before attempting IPR to achieve better access to the interproximal walls. In addition, accomplishing most of the required IPR at the initial visit will increase the accuracy of the reduction. Once teeth are activated for movement, their mobility increases, and it becomes more difficult to determine if the correct amount of reduction has been completed.

Our first step in our IPR protocol is to break all the contacts with the FitStrip Gray 0.05mm (Fig 2) to break open contacts. Reduction between teeth is then accomplished in a step wise fashion starting with the smallest FitStrip and moving towards thicker strips in order to slowly increase the spacing between teeth. In this case, we used the double sided FitStrip Extra Fine Grit Yellow 0.11mm (Fig 3) and Red 0.15mm (Fig 4) in a fine grit. Clinicians can use a TAC topical anesthetic if needed to get the accurate reduction. Hemorrhage is expected with gingival tissue, but patients rarely complain of any discomfort with the reduction when slow, methodical movements are utilized in a controlled fashion. It is also important to note the IPR strip should be tight in the holder which can be adjusted by the colored portion of the handle.
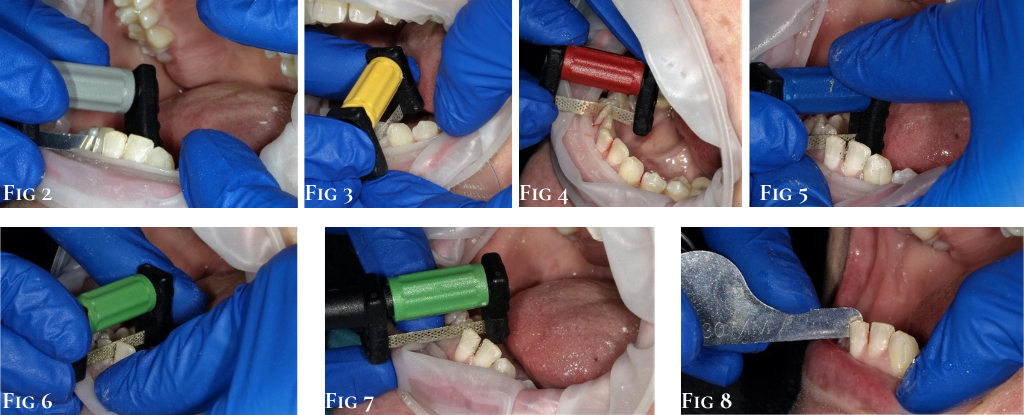
For spaces larger than 0.15mm, the clinician has a choice to decide if they wish to complete the required IPR with hand instruments like the FitStrip or move to rotary instruments or high-speed burs. Hand instrumentation with the FitStrips can also be accomplished if the clinician does not want to utilize rotary instrumentation. FitStrips are available in either a single sided or double sided option and can range in size from 0.08mm to 0.5mm. Clinicians should also note the grit transitions from super fine to medium as the thickness of the strip also increases (Figs 5 and 6). Clinicians can avoid potential hand fatigue with hand instrumentation by utilizing the handle provided in the starter kit. (Fig7) I find that I will alternate using the handle attached to the FitStrips depending on the angulation of the required spacing and my ability to negotiate the reduction safely for the patient’s surrounding tissues and lips.
After reduction is completed per the provided instructions from the clear aligner company, I often go back to the spaces once more with the appropriately sized FitStrip double sided hand instrument to make finishing adjustments and smooth any sharp angles that have resulted from the reduction. A clinician can also use the FitStrip fine grit in 0.15mm to smooth the interproximal sides of the teeth to allow for more ideal approximation during movement. Finally, verify the reduction is completed adequately by using appropriately sized gauge which should slide between the teeth passively indicating the correct reduction has been made. (Fig8). This process is repeated as needed throughout the case in specified intervals depending on the orthodontic plan.
Garrison’s FitStrip system has several advantages over other IPR systems on the market today. Their strips are autoclavable and designed to be used for 20-30 spaces (or approximately 4-6 cases). Our office will take the IPR strips after autoclaving and store them with that patient’s case file. This allows us to continue to use their designated strips throughout their treatment decreasing our overhead on IPR consumables. The FitStrips can also be used to break contacts when cementing veneers and to finish proximal boxes with Class II composites. The ergonomic design of the handle to aid in handling the FitStrip is yet another advantage this system has over many other IPR strips I have tried in my practice.
Protocol Synopsis:
1) FitStrip Gray 0.05mm to break contact
2) FitStrip Yellow 0.11mm and Red 0.15mm double sided
3) FitStrip Blue/Green/Black to finish reduction with hand instruments OR
4) Rotary IPR system to open contacts by 0.2mm-0.5mm
5) FitStrip of appropriate size for reduction to finish the spacing
6) FitStrip IPR gauge to ensure reduction is complete
7) FitStrip Yellow fine grit to smooth the spaces
About the Author
Dr Jennifer Bell is an innovative and fresh voice in the world of dentistry. North Carolinian by birth, with her doctorate from the University of North Carolina, she currently practices in Raleigh NC where she lives with her husband and three children. She introduces a forward thinking perspective to digital innovation, practice management, team building, and leadership development through an engaging and interactive style. Dr Bell is a frequent contributor to leading dental publications, speaks on a variety of relevant and timely topics, and co-hosts a popular, weekly dental industry podcast. Global providers of dental technology, materials, equipment, and other critical services rely on Dr. Bell's input and feedback on new product introductions, marketing strategy, and industry education. She has served as an Advisor, Key Opinion Leader (KOL), and Educator for notable brands like Align Technologies, Benco Dental, Vista Apex, Garrison Dental, and more. She is active in the Academy of General Dentistry, serving on the Dental Practice Council, Government Evaluation and Review Committee and as a national spokesperson. Dr Bell is a valued and highly regarded expert in the field of dentistry.

How long have you been using Sagemax?
I started using Sagemax about three years ago, for as long as Ivodent has been distributor for it here in South Africa.
With regards to colour how true do you find Sagemax?
I would say it’s one of the nearest matching to shade guide colours - about 90-95% true!
Many of the competitors seem to be a little on the bright side how does Sagemax compare?
Sagemax is not bright at all, nowhere near as bright as all the other competitor products.
When looking at milling margin quality and chipping are you happy with Sagemax?
I am very happy indeed and have experienced no chipping problems at all with it!
Have you had many crowns fracture?
I have had the odd one but nowhere near as many as other materials at all.
Does the fact that Sagemax is multilayer give you the option to do full contour anterior restorations or do you do micro layering?
I do both – it depends on each individual case. I either leave as full contour or for extra vitality will go with micro layers.
Does the fact that many of your crowns are full contour save you bench time?
Absolutely – this saves me bench time big time!
Thys tells me he has given you a Sagemax Nexx ZRT to experiment with, how does it compare to the Nexx ZR+?
I actually have not used it yet but I believe it is brighter – I hope to try it out soon! And look forward to it.
Do you need to do micro layering or is the full contour millings sufficient for anteriors? And in the posterior region?
This is case dependant – with multi units I can get away with full contour but for individual aesthetic results then I do micro layering – it’s also shade dependent. For a complicated case with individual Multiple units I can do full contour.
How does the price of Sagemax compare to the competitors?
Sagemax is extremely fairly priced and looking at price vs finished quality - far supersedes the price. One would expect to pay more actually!
Would you recommend Sagemax to your colleagues?
Yes absolutely, I highly recommend it all the time!
Michael Lazarevic purchased Sagemax NexxZr+ Multi from Ivodent.



